The following types of ultrasound are used to assess the pelvic floor:
The transabdominal ultrasound. This approach has the drawback of poor definition and the presence of artifacts, since it must cross many planes in order to reach the pelvic floor musculature.
The transvaginal ultrasound. This approach consists of inserting a transducer into the vagina, thus capturing a 360° image around the probe. Inserting the transducer into the vagina produces some distortion, but it nevertheless provides very good images of the urethral sphincter and the deeper layers of the levator ani muscle (iliococcygeus).
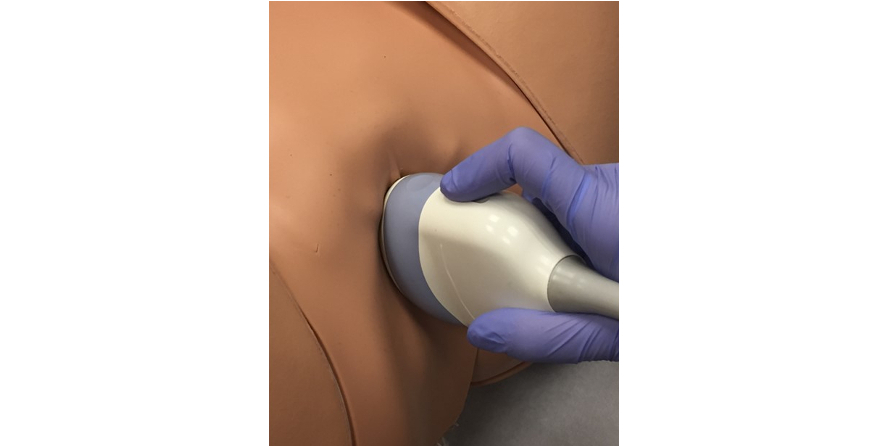
The transperineal or introital ultrasound. This is the most commonly used approach for studying the pelvic floor. The transperineal ultrasound is conducted with the transducer that is usually used for abdominal obstetric ultrasound, resting it on the perineum (Figure 1); the transducer used for the introital ultrasound is the same common sectorial vaginal probe that is used in a vaginal gynaecological ultrasound, but in this case the probe simply rests on the suburethral area (Figure 2). This approach has the advantage of low distortion; the small degree of distortion that it does produce can be avoided by regulating the pressure of the transducer on the area. The transperineal and introital ultrasound routes are the most comfortable approaches, seeing as they do not require entering the vagina and they allow for a good assessment of all three compartments of the pelvic floor: the anterior, middle and posterior. They even allow us to see, distortion-free, the anal mucosa and the external and internal anal sphincter.
The endoanal ultrasound. This approach employs the same 360° transducer as the transvaginal ultrasound, but in this case, the probe is introduced through the anal canal. It is considered the gold standard technique for diagnosing anal sphincter injury. This approach obviously causes both distortion and discomfort.
Figure 1. The transperineal ultrasound is the most frequently used approach