The levator ani muscle and its involvement in childbirth
The levator ani muscle is a muscular structure that comes together in the lower part of the bony pelvis, but its function is not only that of supporting the pelvic organs; it is also involved in basic functions of the human species, such as continence-urination and continence-defecation, sexuality and pregnancy and childbirth. In the case of pregnancy and childbirth, the levator ani muscle, which comprises the urogenital hiatus, will undergo a process of spectacular elongation in order to allow for the fetus to pass through the birth canal.
For a long time, the greater or lesser impact of childbirth on this muscular structure proposed relatively little concern for most professionals. Many patients even live with pelvic floor pathology as though it were intrinsic to motherhood. Fortunately, this has been changing in recent years, stemming from more precise anatomo-physiological knowledge of this pathology as well as biomechanical studies of childbirth and the emergence of pelvic floor pathology units.
One of the most prominent professionals who has contributed to the knowledge of this pathology is Dr. John DeLancey, who has helped us perceive the levator ani muscle as the extremely important functional structure that it is (1). The different fascicles of the levator ani muscle - the ileococcygeus and the puborectalis-pubovisceral - have been studied in detail in order to understand their involvement in pelvic floor pathology. The stretch that this muscular structure undergoes during childbirth cannot be compared with that of any other muscular structure of the human anatomy. How this muscle endures such a stretch can be understood by examining its biophysical characteristics; viscoelasticity is probably one of the most important aspects that allows the muscle fibre to progressively lengthen without suffering damage. Despite this elongation of the fibres, sometimes they nevertheless end up detaching themselves from their pubic bone anchor, thus resulting in a levator ani injury.
The most frequent mechanism of the onset of prolapse is the levator ani injury, which involves the opening of the urogenital hiatus. When the pelvic structures lose their most important support, the fascia structures that support the bladder and uterus will progressively elongate. This elongation, encouraged by the pull of gravity, causes the vaginal vault, as well as the uterus and bladder, to descend towards the urogenital hiatus.
Another mechanism of injury, independent of the levator ani injury, may be a fascia injury, but it is much more infrequent. This injury can be assessed using TUI through a three-dimensional ultrasound (2).
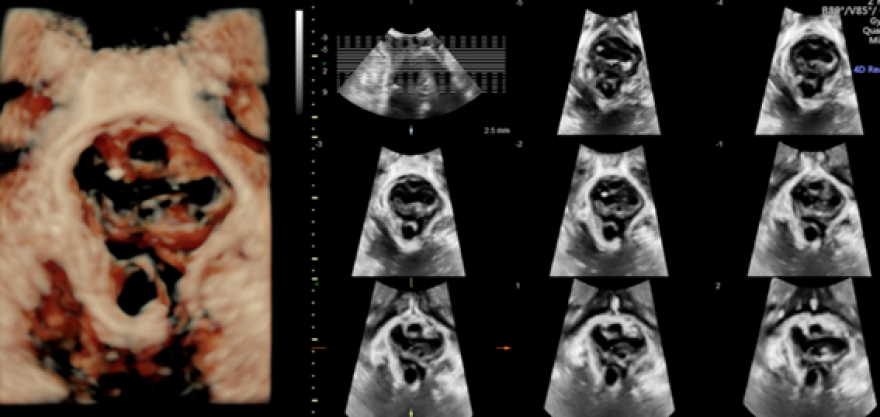
As we mentioned, muscular injury is both the most significant and the most frequent type of injury. Ultrasonographically, it is described as a macro or microtrauma (3). Macrotrauma, or avulsion, refers to the direct detachment of the puborectal-pubovisceral fascicle of the levator ani from the pubic symphysis (Figure 1).
Figure 1. On the left, a left injury of the levator ani is pictured in a three-dimensional image; on the right we have the same image assessed using TUI on the three central slices (avulsion)
A microtrauma consists of the pathological enlargement, or hyperdistension, of the urogenital hiatus, with an area greater than 25 cm² when performing the Valsalva manoeuvre. This excessive distension is also called "ballooning".
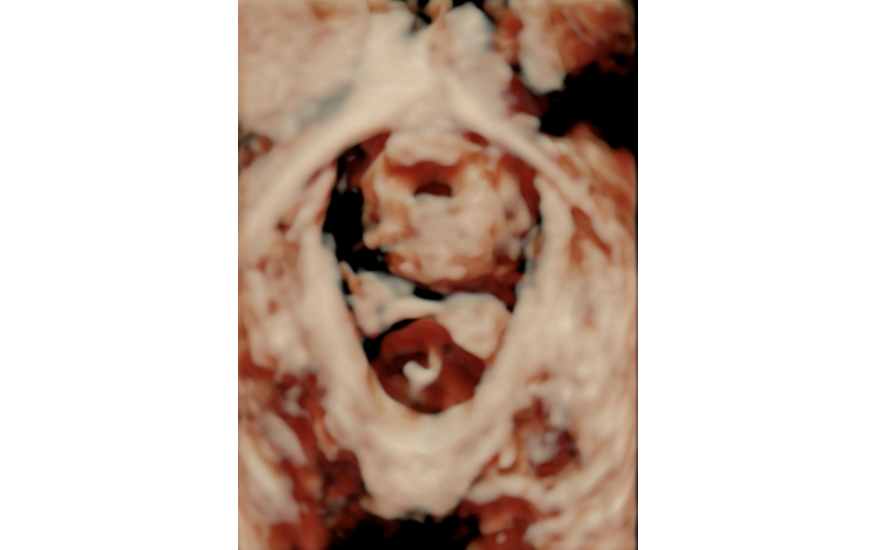
Figure 2. The image depicts a normal urogenital hiatus area (A).
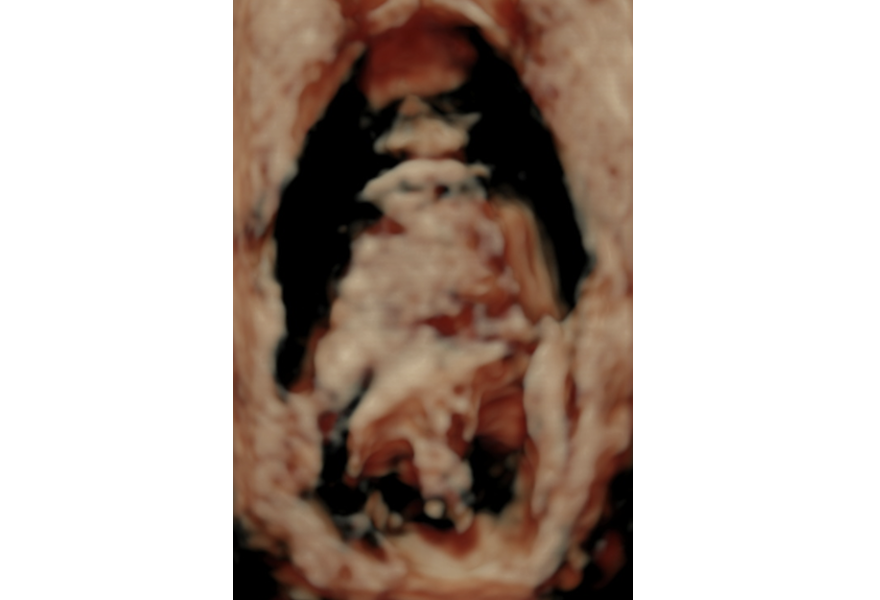
Figure 3. Enlarged urogenital hiatus
Levator ani injury can be studied by TUI using the assessment of the three central slices (shown in Figure 1), as explained in the Technical and methodological aspects section, as well as by measuring the distance from the urethra to the levator ani's first fibres; the latter is a very objective way of assessing the injury (any distance greater than 25 mm suggests injury) (4).
Muscle injury can also be assessed by two-dimensional ultrasound with acceptable correlation, as some authors have indicated; it is, however, much more difficult (5).
But what is the significance of these injuries?
The significance of these injuries is mainly prognostic, given that an enlarged urogenital hiatus is an independent risk factor for the onset of genital prolapse. On the other hand, levator ani injury – macrotrauma – is associated twice as much with the emergence of genital prolapse and also with the risk of recurrence after conventional surgery (3). Although these injuries clearly influence the onset of prolapse, they do not seem to be directly related to urinary or faecal incontinence, despite sharing risk factors.
Studies on the risk factors associated with the onset of levator ani injury have found that one of the most important factors involves the instruments used during childbirth, especially the use of forceps, which is associated with a levator ani injury risk with a ratio of 14.7 (6). Forceps are well designed for the fetus and the birth canal – that is, the bony birth canal. Factors that could contribute to this injury include the increase in diameter upon the insertion of the forceps, as well as the loss of viscoelasticity in the untimely traction used for extracting the fetal calvaria. Many authors have shed light on the assessment of levator ani injury using three-dimensional ultrasound. In a study of 180 patients, our group detected a rate of avulsion of 61.7% in deliveries with forceps and only 13.3% in eutocic deliveries (7). In a recent systematic review, most authors obtained similar results (8).
Although other intrapartum factors that may also be related to the levator ani injury have been described, according to a multivariate analysis of the data, the most influential factor tends to be that of instrumental delivery, regardless of the reason for which it was indicated – both due to suspected loss of fetal well-being or stalled labour. It seems that rotational forceps are the most harmful. The percentage of injury associated with other instruments, such as the vacuum extractor, is much lower than that of the forceps. The prevalence of avulsion with forceps triples that of the vacuum (9).
One of the most concerning aspects of diagnosing levator ani injuries is the presence of false images. Attempts have been made to minimize false images by using Doppler technology, but more studies are still needed (10).
When fewer than three slices are involved in the TUI of the levator ani injury, we are dealing with a partial injury, which does not have as much impact as a complete injury (11).
Although there is a certain potential for recovery following any type of childbirth, in the case of levator ani injury, it is difficult to recover 100% of the muscle's functionality. Studies using resonance imaging have demonstrated that patients can recover from bone injuries and the oedema that sometimes occurs at the pubic symphysis after childbirth, but that they do not fully recover from levator ani injuries.
There are some studies in which the prolapse symptom of levator ani injury does not present itself within a year of the injury, but we must also bear in mind that these injuries often take years to manifest. Latency of 33.5 years has been established (ranging from 3 to 66 years in a recent retrospective observational study). Maternal age and the use of forceps during delivery decrease the period of latency (12).
In addition, we must bear in mind that prolapse depends not only on levator ani injury, but also on many other factors previously discussed here, including: pure fascial defects, paravaginal defects (2), the emergence of neurological injuries, recto-vaginal septum injuries (which would explain the origin of posterior compartment prolapse) and injuries of other little-studied fascicles, such as the anterior part of the pubovisceral muscle. Avulsion and levator ani injury are very easy to diagnose, both clinically and by ultrasound.
Regarding prevention, we know that episiotomy has little effect on levator ani injury: in studies of eutocic deliveries, the percentage of levator ani injury with or without episiotomy is the same (13, 14). Perineal massage is associated with a lower incidence of episiotomies, but it does not make a difference in the rate of instrumental deliveries or in the incidence of urinary and faecal incontinence, gas or in terms of sexual satisfaction. Devices such as EPI-NO do not seem to be associated with a lower incidence of levator ani injury (15). Given that body mass index seems to be a risk factor for levator ani injury, it should be strictly monitored before delivery, since it is one of the few aspects through which we can manage primary prevention. However, a very important part of prevention lies in establishing changes in obstetric habits: changes in favour of using the vacuum extractor, rigorous indications for the use of instruments and changes in teaching methods. Fortunately, there are birth simulator mannequins for learning how to correctly use both the vacuum extractor and forceps.
In the future, we must be able to identify patients who present the possibility of levator ani injury in order to consider less traumatic delivery options in these high-risk patients; that said, we still need more studies on this topic in order to be able to draw clinically applicable conclusions.
We can conclude that: the use of forceps increases the risk of levator ani injury more than that of the vacuum extractor; levator ani injury is a risk factor associated with prolapse but is probably not the only one; and we need new teaching methods and improvements in the diagnosis of these types of injuries. Our current knowledge indicates that it is high time to prevent and minimize the impact of childbirth on women.
Bibliography
DeLancey JO, Morgan DM, Fenner DE, Kearney R, Guire K, Miller JM, Hussain H, Umek W, Hsu Y, Ashton-Miller JA. Comparison of levator ani muscle defects and function in women with and without pelvic organ prolapse. Obstet Gynecol 2007;109:295–302.
Cassadó-Garriga J, Wong V, Shek K, Dietz HP. Can we identify changes in fascial paravaginal supports after childbirth? Aust N Z J Obstet Gynaecol. 2015;55:70-75.
Dietz HP, Simpson JM. Levator trauma is associated with pelvic organ prolapse. BJOG. 2008;115:979–984.
Dietz HP, Abbu A, Shek KL.The levator-urethra gap measurement: a more objective means of determining levator avulsion? Ultrasound Obstet Gynecol 2008;32:941-5.
Dietz HP, Shek KL. Levator defects can be detected by 2D translabial ultrasound.Int Urogynecol J Pelvic Floor Dysfunct. 2009;20:807-11
Kearney R, Miller JM, Ashton-Miller JA, DeLancey JO. Obstetric factors associated with levator ani muscle injury after vaginal birth. Obstet Gynecol. 2006;107:144-149.
Cassadó Garriga J, Pessarrodona Isern A, Espuña Pons M, Duran Retamal M, Felgueroso Fabrega A, Rodriguez Carballeira M, Jordà Santamaria I. Four-dimensional sonographic evaluation of avulsion of the levator ani according to delivery mode. Ultrasound Obstet Gynecol. 2011;38:701-706.
Dietz HP, Wilson PD, Milsom I. Maternal birth trauma: why should it matter to urogynaecologists? Curr Opin Obstet Gynecol. 2016;28:441-448.
Memon HU, Blomquist JL, Dietz HP, Pierce CB, Weinstein MM, Handa VL. Comparison of levator ani muscle avulsion injury after forceps-assisted and vacuum-assisted vaginal childbirth. Obstet Gynecol. 2015;125:1080-1087.
Cassadó Garriga J, Quintas Marques L, Pessarrodona Isern A, López Quesada E, Rodriguez Carballeira M, Badia Carrasco A. Can 3D Power Doppler identify levator ani vascularization at its pubic insertion?. Int Urogynecol J 2015;26:1327-32.
Dietz HP, Bernardo MJ, Kirby A, Shek KL. Minimal criteria for the diagnosis of avulsion of the puborectalis muscle by tomographic ultrasound.Int Urogynecol J 2011;22:699-704.
Thomas V, Shek KL, Guzman Rojas R, Dietz HP. Temporal latency between pelvic floor trauma and presentation for ptolapse surgery: a retrospective observational study. Int Urogynecol J 2015;26:1185-89.
Cassadó J, Pessarrodona A, Rodriguez-Carballeira M, Hinojosa L, Manrique G, Marquez A, Macias M. Does episiotomy protect against injury of the levator ani muscle in normal vaginal delivery? Neurourol Urodyn 2014;33:1212-1216.
Cassadó Garriga J, Carmona Ruiz A, Pessarrodona Isern A, Rodríguez Carballeira M, Esteve Serena E, García Manau P, Valls Esteve M, Huguet Galofré E. Impact of episiotomy on the urogenital hiatus using transperineal ultrasound. Neurourol Urodyn 2018;37:434-439.
Kamisan Atan I, Shek KL, Langer S, Guzman Rojas R, Caudwell-Hall J, Daly JO, Dietz HP.pèlvic (Does the Epi-No(®) birth trainer prevent vaginal birth-related pelvic floor trauma? A multicentre prospective randomised controlled trial. BJOG 2016;123:995-1003.